Adult Attention Deficit Hyperactivity Disorder (ADHD): To what extent do comorbid diagnosis occur with Adult ADHD? What are the implications of diagnosis and treatment options for participants living in Tasmania.
SOCA311 – Research Project
Student: Heather Beamish – 260117
Word Count: 2226
Due: 20/05/2022
Title:
Adult Attention Deficit Hyperactivity Disorder (ADHD): To what extent do comorbid diagnosis occur with Adult ADHD? What are the implications of diagnosis and treatment options for participants living in Tasmania.
Introduction and theoretical framework
Attention Deficit Hyperactivity Disorder (ADHD) is characterised by problems with attention and behaviour related to eight (8) executive functions, which are “working memory, planning / organising, task monitoring, self-monitoring, inhibition, shifting between activities, emotional control and initiation”, (ADHD Australia, 2022). Physiologically, differences in the ADHD brain are visible with Magnetic Resonance Imaging (Bush et al, 2008). ADHD Australia.org reports that, “ADHD affects approximately 281,200 children and adolescents (0-19 years old) and 533,300 adults in Australia (20+ years old)”. It is not yet known whether the ADHD brain can change via neuroplasticity, however studies are emerging that report various practices may help in regards to improving executive functioning, for example, Mindfulness Meditation Training (Mitchell et al, 2015).
A database search of co-existing factors affecting Adults with ADHD, formed the basis for this investigation. The aim of this study is to expand on existing ADHD studies by Surveying Adult participants with ADHD in Tasmania. Each topic of research questions, will be organised into four main categories:
1. Does the participant have a coexisting psychiatric diagnosis alongside ADHD
2. Does the participant have access to Biomedical (Biomed) and or Complementary and Alternative Therapies (CAM)
3. What are the participant’s experiences of diagnosis and the effects of the diagnosis on their lifestyle and Social Determinants of Health (SDH)
4. Is the participant experiencing a Substance Use Disorder (SUD) / or have they experienced a SUD.
Statement of the problem
Not a lot is known about the cause of ADHD though there is evidence that both Genes and the Environment are involved (ADHD Australia, 2022). Additionally, there is often a co-morbid diagnosis that occurs where a person has ADHD (Gentile et al, 2006). There may be at a higher risk with ADHD of experiencing other mental health conditions such as major depressive disorder (MDD), generalised anxiety disorder (GAD), bipolar disorder (BP), borderline personality disorder (BPD), substance use disorder (SUD), or another diagnosis (Gentile et al, 2006’, Gnanavel et al, 2019., Gonzalez et al, 2020., Sherman et al, 2021). More information needs to be researched, as to why there are higher mental health risks associated with ADHD, and as to which interventions, or educational strategies, as an example, could be of help for more succesful health outcomes for those with ADHD, and or co-existing diagnosis. SDH also comes into focus here. With more knowledge, public health professionals and community workers can subsequently be better equiped to provide helpful services to clients.
Purpose of the study
The purpose of the study is to gain more of an understanding of Adult ADHD in relation to existing evidence. The cohort of people interviewed with adult ADHD will be in Tasmania. Participants will be asked to self-report on their experiences of ADHD and or other diagnosis, in their lives. Their reflection and reporting will be guided by survey questions relating to existing research to gain more understanding of the effects of ADHD in Tasmanian participants. The data collected aims to be a useful and helpful inclusion to the growing body of research and knowledge about Adult ADHD.
Question or hypothesis/hypotheses
From existing research findings, it’s expected that this study will show diagnosed co-morbid disorders occurring in addition to the diagnosis of ADHD (Katzman et al, 2017). The majority of participants will likely manage their diagnosis with an Integrative approach, as many Australians utilise a combination of Biomed and CAM approaches for their health care (Von Conrady & Bonney, 2017). SDH will affect the types of treatment options chosen by participants and the study will show correlations between these (Islam M, 2019). It’s also possible that there will be history of SUD (past or present) due to maladaptive coping strategies either before diagnosis, or as a result of trauma or other lifestyle challenges (González, et al., 2020., Young and Woodhouse, 2021).
Significance
Well known ADHD treatment approaches currently involve taking pharmaceutical medications and undertaking therapy (Caye et al, 2019., Sherman et al, 2021). CAM approaches are also often utilised (Sarris et al, 2011). A unique set of circumstances come along with each diagnosis. While the essential characteristics of ADHD in people all over the world are the same in regards to experiences related to the 8 executive functions (ADHD Australia, 2012., Brod et al 2012), there are multifactorial inputs to consider, when a person chooses their treatment approaches; for example affordability of treatment, waiting lists to treatment, tolerability of medications, and personal preferences, skillsets, and beliefs when it comes to wellness choices (Zylowska, 2022). Public health knowledge and support for ADHD can improve where there is a greater evidence base to show that further research and even wellness strategies related to this are worth the time and funding.
Literature review
For this enquiry data base searches were utilised including Google scholar, Ebsco, and Discovery, to search Adult ADHD. Key themes that emerged from this search were: ADHD and co-morbid diagnosis, ADHD and CAM, ADHD and Social Determinants of Health, ADHD and Substance Use. A review of approximately 15 articles was undertaken, relating to four categories, developed to further design research questions (see Appendix pg. 16-18). Other articles mentioned here have also been referenced in text.
Of the research findings, Biomed treatment currently has a large evidence base (Bush et al, 2008., Champ et al, 2021., Russell et al, 2016). This approach prescribes medication and therapy practices including Cognitive Behavioural Therapy (CBT) and in some cases Dialectical Behavioural Therapy (DBT) (Cole, et al., 2016., Sherman et al, 2021). From the view of an Integrative medical approach, the evidence base was less, though the articles showed good evidence that CAM is also of help. It’s expected that a wider search would return more evidence. Mindfulness Practices came up in the search as being useful in the treatment of ADHD as well (Rucklidge et al, 2009., Mitchell et al, 2015., Sarris et al., 2011). There is good evidence to show that nutritional and herbal approaches including supplementation of foods or multi vitamin and mineral tablets containing: “zinc, iron, omega-3, vitamin C, or acetyl-l-carnitine” may help (Sarris et al, 2011). Herbal supplements such as, Ginkgo biloba (ginkgo), Ningdong Granule and Rehmanniae radix preparata also show some efficacy, (Brue et al, 2002., Rucklidge et al, 2009., Sarris et al, 2011., Yuan et al, 2018).
The different SDH come into focus when looking at ADHD and other diagnosis. Self management and coping skills with regards to wellness is a big component of succesful health outcomes (Burnette et al, 2020., Zylowska, 2022). In a small study by Canela et al (2017), “Skills and Compensation Strategies of Adults with ADHD”, the research team interviewed 32 people about the life skills they’d developed before diagnosis and treatment. Many participants had already developed helpful skillsets including the use of electronic calender reminders, following set routines, and undertaking self help research to better understand their learning and communication styles as examples; many had taught themselves how to prioritise time for their wellbeing in overcoming the additional life challeges they faced with ADHD. The study concluded that health pracitioners may find it useful to get to know their clients coping mechanisms individually, and follow a more client led treatment plan, rather than blindly following a standard treatment regimine. This may lead to better health outcomes and patient cooperation.
Methodology
This study will inform participants of the four categories of research (see table 1. pg. 9-11) in the call out to participate. When people register, they will be sent a confidentiality agreement and informed consent form. The names and contact details of the participants will be recorded and kept for follow up to the study at 1, 3 & 5 years, but the survey itself will be anonymous. It will be open for 3 months initially. Participants will need to set aside a stretch of time (e.g. up to an hour) to reflect on the questions and give their answers. There will be a space provided to write short or long answers to questions. Some questions will be Yes, No, and Multi-Select.
The survey aims to gain insight and a broad understanding of the types of issues that participants face in their daily lives. If a participant requires assistance such as an interpreter, literacy or numeracy support, or access to a computer and internet, this can be provided by the research team; or the option of a face to face interview, which may be made by appointment if better suited for the participant. Further details are as follows:
Participants
Participants from Tasmania will be invited. The study aims to Survey 200 + People with a diagnosis of ADHD
Recruitment
Researchers will write to the University of Tasmania, Community Centres, Health Centres, The Complementary Medicine Association (to invite Tasmanian members), and the Hobart ADHD Clinic.
Sampling
The researchers and participants will be given the four categories of questions before volunteering / registering – and will have a 3-month window to complete the survey. A contact person and phone number for the research team will be provided. Participants must register with their name, phone number, and email address, and state their preferences for participation (internet survey link, phone, interpreter, or in person). They will then be contacted to sign a confidentiality agreement and consent form, and to take the next step of completing the survey anonymously. During the time the survey is open, researchers will again contact participants to remind them of the closing date and ask them if they need any assistance.
As previously stated, the questions will invite participants to write / or speak freely to minimise interpretation bias. Where participants would prefer to hold a confidential in person interview, researchers will use voice transcription software and also write answers with the participant. The survey should take approx. 1 hour to complete.
Inclusion / Exclusion Criteria
To meet the study requirements a person must be over the age of 18 and have a diagnosis of ADHD. There are no specific exclusion criteria.
Data Collection Recording Formats, Data Analysis, and Outcome Measures
Survey data will be collected (via survey, phone, writing, or voice recording) and transcribed with Computer Assisted Qualitative / Quantitative Data Analysis Software (CAQDAS). Researchers will meet on Zoom monthly during the survey to troubleshoot problems, and again after the study to collate information. The ‘Framework Analysis’ (Gill et al, 2008) will be used to analyse, code, and transcribe research data.
Reporting/Results and Discussion
This research will add to the existing knowledge base of ADHD and so assist health professionals to adapt their treatment approaches to Adults with ADHD over time. The variables of this study are the participation and level of detail given by participants. Also, it’s not possible to screen participants for their diagnosis. Some people might participate without a diagnosis. This will be discouraged at registration. This research aims to detail the issues affecting this cohort of people living with ADHD in Tasmania.
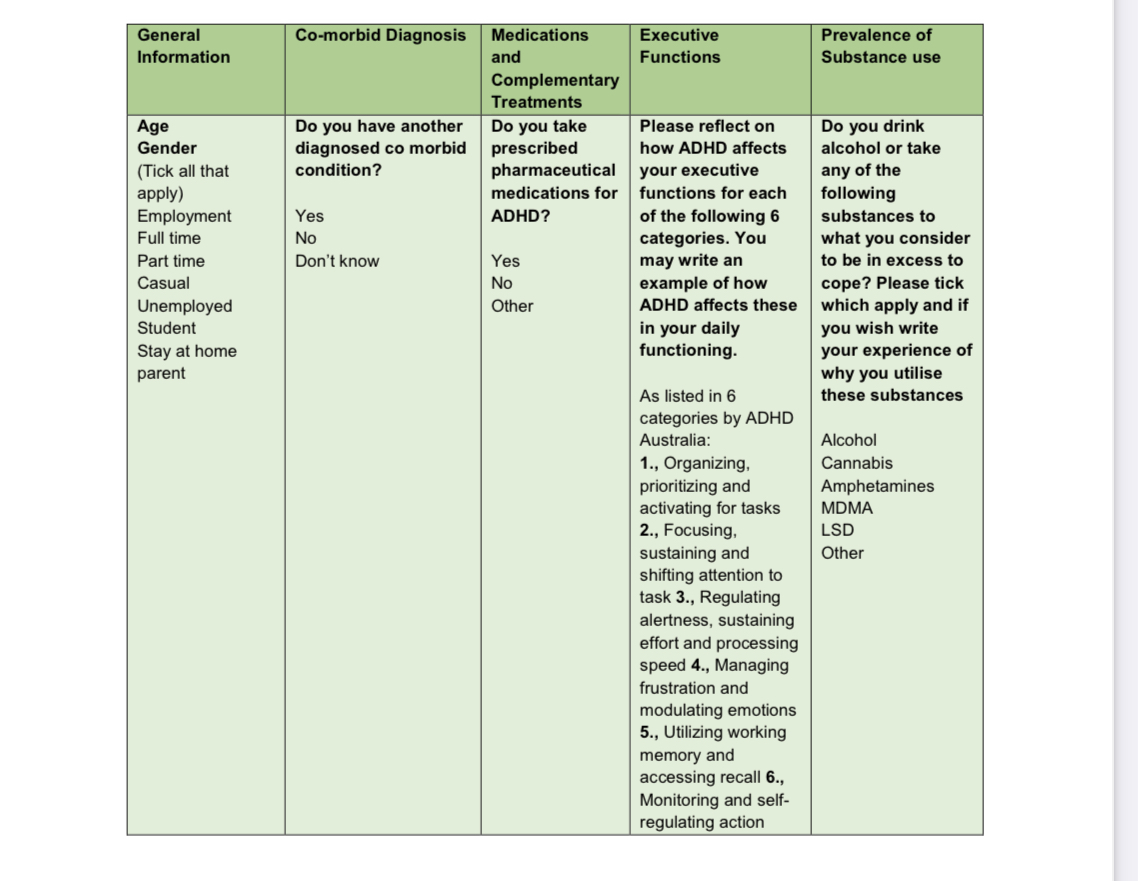
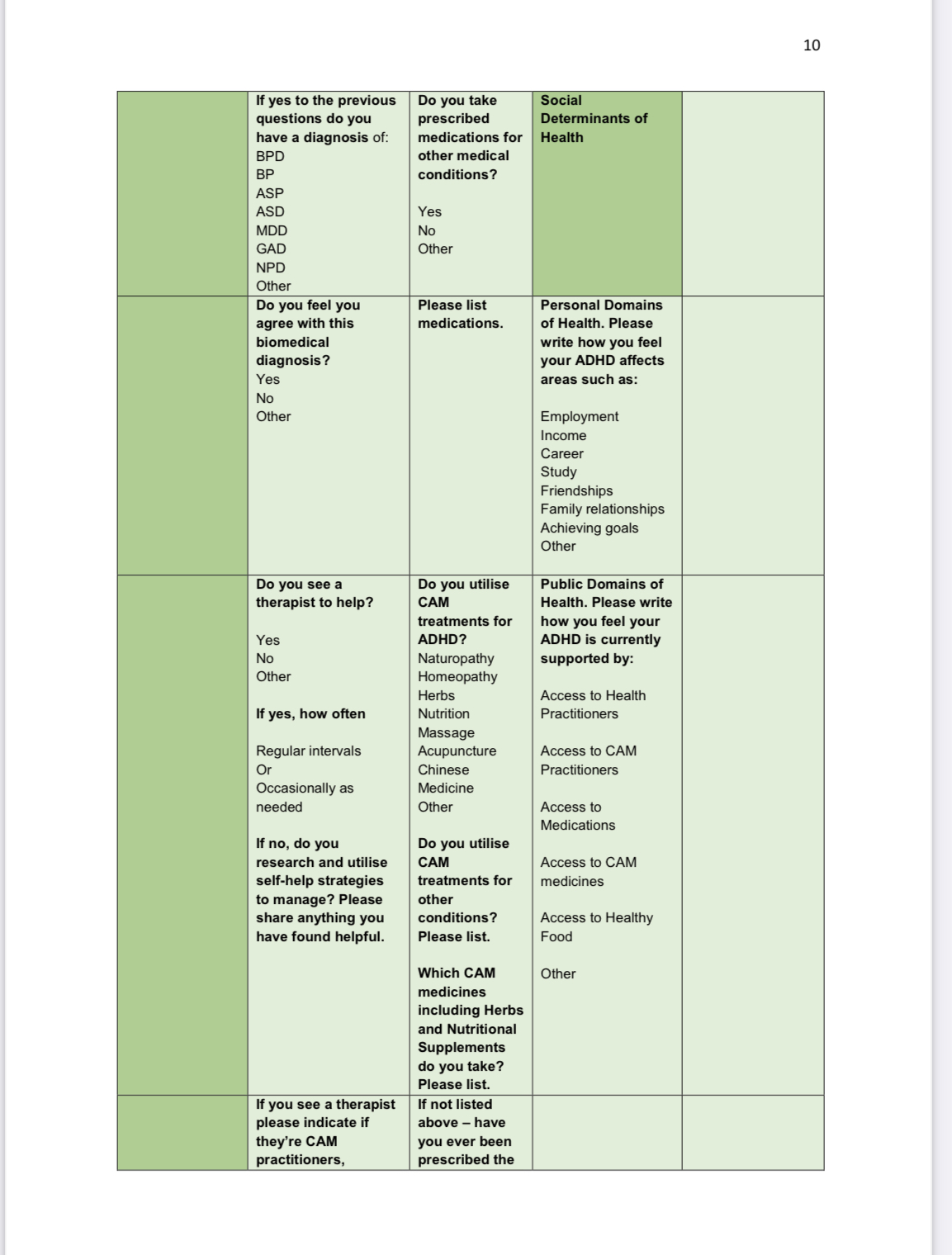
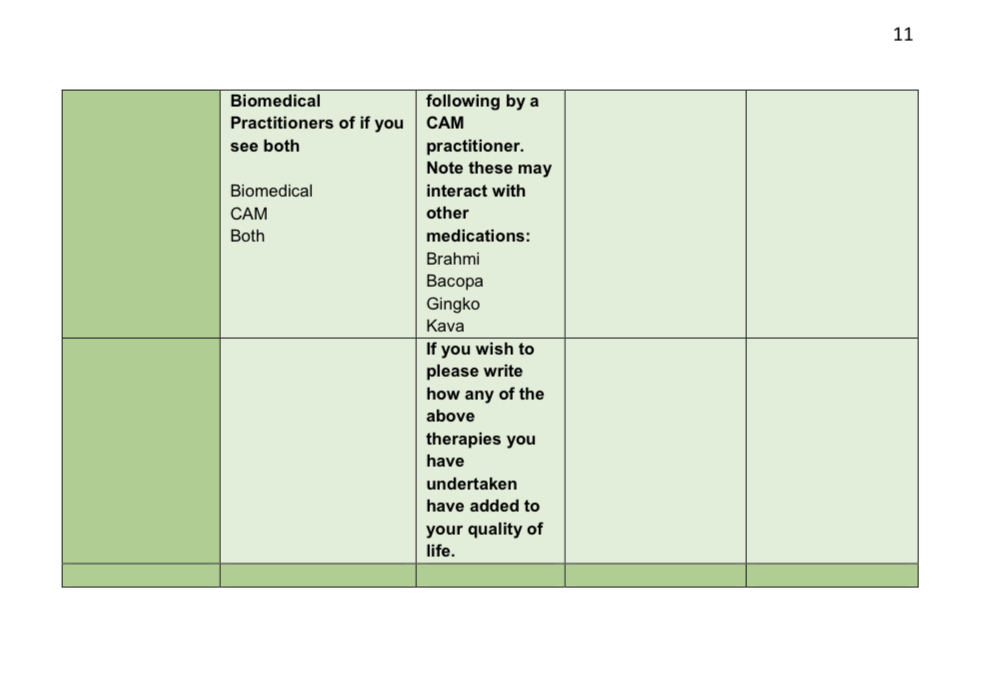
If successful, this research and survey results may be submitted to organisations such as ADHD Australia.org or the Complementary Medicine Association of Australia. More research is needed to ascertain which journals will accept research by independent researchers and students. See table 1. Below, for a description of the survey questions to be formatted for participants.
Table 1 Research Methodology – Survey Questions to be formatted
References
ADHD Australia. (2022). ADHD Australia. Retrieved from https://www.adhdaustralia.org.au/get-involved/
Brandt, L., Levina , F., & Kraigher, D. (2021). Impulsive Personality Traits Mediate the Relationship Between Attention-Deficit/Hyperactivity Disorder Symptoms and Psychiatric Comorbidity among Patients with Severe Alcohol Use Disorder. Journal of Duel Diagnosis. doi:https://doi.org/10.1080/15504263.2021.1944711
Burnette, J. L., Babij, A. D., Oddo, L. E., & Knouse, L. E. (2020). Self Regulation Mindsets – Relationship to Coping, Executive Function and ADHD (Vols. Vol. 39, No. 2). Journal of Social and Clinical Psychology. doi:https://doi.org/10.1521/jscp.2020.39.02.101
Bush, G., Spencer, T., & Holmes, J. (2008). Functional Magnetic Resonance Imaging of Methylphenidate and Placebo in Attention-Deficit/Hyperactivity Disorder During the Multi-Source Interference Task (Vol. 65:1). Arch Gen Psychiatry. doi:10.1001/archgenpsychiatry.2007.16
Canela, C., Buadze, A., Dube, A., Eich, D., Liebrenz, M., & Chao, L. (2017). Skills and compensation strategies in adult ADHD – A qualitative study (Vol. 12:9). PLoS One. doi:https://dx.doi.org/10.1371%2Fjournal.pone.0184964
Caye, A., Swanson, D., Coghill, D., Rhode, L.A. (2019).Treatment strategies for ADHD: an evidence-based guide to select optimal treatment (Vols. 24, Iss. 3 ) Journal of Molecular Psychiatry. doi:DOI:10.1038/s41380-018-0116-3
Cole, P., Weibel, S., Nicastro, R., Hasler, R., Dayer, A., Aubry, J.-M., . . . Perroud, N. (2016). CBT/DBT skills training for adults with attention deficit hyperactivity disorder (ADHD). Psychiatria Danubina.
E. Champ, R., Adamou, M., & Tolchard, B. (2021). The impact of psychological theory on the treatment of Attention Deficit Hyperactivity Disorder (ADHD) in adults: A scoping review. (Vol. 16 Issue 12). Plos One.
Frodl, T., & Skokauskas, N. (2011). Meta-analysis of structural MRI studies in children and adults with attention deficit hyperactivity disorder indicates treatment effects. Retrieved from https://doi.org/10.1111/j.1600-0447.2011.01786.x
Gentile, J., Atiq, R., & Gillig, P. (2006). Adult ADHD Diagnosis, Differential Diagnosis, and Medication Management. Psychiatry (Edgmont).
Gill, P., Stewart, K., Treasure, E., & Chadwick , B. (2008). Methods of data collection in qualitative research: interviews and focus groups (Vol. 204). British Dental Journal.
Gnanavel, S., Sharma, P., Kaushal, P., & Hussain, S. (2019 Sep). Attention deficit hyperactivity disorder and comorbidity: A review of literature (Vol. 6; 7:17 2). World J Clin Cases. doi:https://dx.doi.org/10.12998%2Fwjcc.v7.i17.2420
González, R., Vélez-Pastrana , M., Blankers , M., Bäcker , A., Konstenius, M., Holtmann , M., . . . Schellekens, A. (2020). Onset and Severity of Early Disruptive Behavioral Disorders in Treatment-Seeking Substance Use Disorder Patients with and without Attention-Deficit/Hyperactivity Disorder (Vol. 26). Eur Addict Res. doi:https://doi.org/10.1159/000508653
Hurt, E., Lofthouse, N., & Arnold, E. (2010). Complementary and Alternative Biomedical Treatments for ADHD. Psychiatric Annals.
Islam, M. (2019). Social Determinants of Health and Related Inequalities: Confusion and Implications. Frontiers in Public Health.
Katzman, M., Bilkey, T., Chokka, P., Fallu,, A., & Klassen, L. (2017). Adult ADHD and comorbid disorders: clinical implications of a dimensional approach (Vol. 7). BMC Psychiatry.
Lake, J., & Sarris, J. (2019). Complementary and Alternative Treatments for ADHD: What the Evidence Suggests (Vols. 36, Issue 10). Psychiatric Times. Retrieved from https://www.psychiatrictimes.com/view/complementary-and-alternative-treatments-adhd-what-evidence-suggests
Letkiewicz, A., Miller, G., Crocker, L., Warren, S., Infantolino, Z., Mimnaugh, K., & Heller, W. (2014). Executive Function Deficits in Daily Life Prospectively Predict Increases in Depressive Symptoms. New York: Springer Science+Business Media.
Mitchell, J., Zylowska, L., & Kollins, S. (2015). Mindfulness Meditation Training for Attention-Deficit/Hyperactivity Disorder in Adulthood: Current Empirical Support, Treatment Overview, and Future Directions (Vol. 22:2). Cognitive Behavioural Practices. doi:10.1016/j.cbpra.2014.10.002
Rucklidge, J., Johnstone, J., & Kaplan, B. (2009). Nutrient supplementation approaches in the treatment of ADHD (Vols. 9, Iss. 4 ). Expert Review of Neurotherapeutics. doi:10.1586/ern.09.7
Russell Ramsay, J. (2002). Is There a Cognitive Theme to the Thoughts and Beliefs of Adults with ADHD?
Russell Ramsay, J., & Rostain, A. (2016). Adult Attention-Deficit/Hyperactivity Disorder as an Implementation Problem: Clinical Significance, Underlying Mechanisms, and Psychosocial Treatment.
Sarris, J., Kean, J., Schweitzera, I., & Lake, J. (2011). Complementary medicines (herbal and nutritional products) in the treatment of Attention Deficit Hyperactivity Disorder (ADHD): A systematic review of the evidence (Vol. 19). Elsevier.
Sherman, C., Ramsay, R., & Barrow, K. (2021). CBT is supported by clinical results and research evidence showing that the therapy delivers real-world benefits for adults with ADHD — namely higher self-esteem, productivity, and happiness. ADDitude – Inside the ADHD mind.
Sherman, J., & Tarnow, J. (2013). What Are Common Comorbidities in ADHD? (Vol. 30: 8 ). Psychiatric Times.
Von Conrady, D. M., & Bonney, A. (2017). Patterns of complementary and alternative medicine use and health literacy in general practice patients in urban and regional Australia (Vol. 46:5). Australian Family Physician. Retrieved from https://www.racgp.org.au/afp/2017/may/patterns-of-complementary-and-alternative-medi-2#:~:text=Complementary%20and%20alternative%20medicine%20%28CAM%29%20has%20become%20an,whereas%20%E2%80%98alternative%E2%80%99%20is%20taken%20to%20mean%20instead%20of.
Young, S., & Woodhouse, E. (2021). Assessment and treatment of substance use in adults with ADHD: a psychological approach (Vol. 128). Journal of Neural Transmission.
Yuan, H., Meng, Y., Han, X., & Ni, X. (2018). The Therapeutic Effect of the Chinese Herbal Medicine, Rehmanniae Radix Preparata, in Attention Deficit Hyperactivity Disorder via Reversal of Structural Abnormalities in the Cortex. Evidence Based Complementary and Alternative Medicine.
Zylowska, L. (2022). What Is Integrative Medicine for ADHD? A Holistic Health & Wellness Guide. ADDitude.
Appendix
Appendix table. Literature Review – Background Research to Study Design